THYROID NODULES
(ULTRASOUND)
Last modified: September 6, 2025
Main reference: TIRADS 2017

Target population
Exclusion
High risk of thyroid carcinoma
Symptomatic dysthyroidism
<18 years old
Definitions
TRUE ANEURYSM
Permanent dilation exceeding 50% of the normal diameter, involving all layers of the wall (intima, media, adventitia).
PSEUDOANEURYSM
Perivascular collection communicating with the arterial lumen, contained only by the surrounding tissues. Significantly higher risk of rupture.
VISCERAL ANEURYSM
Aneurysm of a visceral artery: splenic, hepatic, SMA, celiac, renal, pancreaticoduodenal or gastroduodenal.
Important Notes
Symptomatic pseudoaneurysms and aneurysms: refer to vascular surgery immediately, regardless of size or location. A pseudoaneurysm does not benefit from any period of observation.
AMS, pancreaticoduodenal and gastroduodenal: vascular surgery consultation required immediately, regardless of size. High prevalence of mycotic origin and higher risk of rupture compared to other visceral territories.
Women of childbearing age (not just pregnant): for renal and splenic aneurysms, consult a vascular surgeon even below the usual thresholds. The risk of rupture is almost fatal for both the mother and the fetus. Prophylactic embolization is often performed.
Differences between SVS and CIRSE: SVS uses a 3 cm threshold for the renal and splenic arteries; the European CIRSE uses 2 cm. This guide is based on the 2020 SVS guidelines.
Hepatic aneurysm > 5 cm with comorbidities: consultation with a vascular surgeon is still recommended; embolization is feasible with low procedural risk. Maintaining outpatient follow-up without vascular evaluation carries significant risks.
Additional Notes
Risk of neoplasia
TI-RADS 1: < 2%
TI-RADS 2: < 2%
TI-RADS 3: 5%
TI-RADS 4: 5 to 20%
4 points: 6%
5 points: 10%
6 points: 13%
TI-RADS 5: ≥ 20%
Report 3 dimensions of the nodule
Include nodule halo if present
Recommendation according to longest diameter
No ultrasound follow-up for <1 year
Except for proven cancer requiring monitoring
If nodule already biopsied, classify TIRADS on ultrasound as usual
No specific recommendations in the report
Mention that management should be at least partly guided by biopsy results
If the nodule has already been biopsied with benign pathology and continues to increase on ultrasound,
According to ATA 2015, highly suspicious nodule should be followed up by ultrasound and cytology if necessary
Follow-up may be >5 years if remains below cytology threshold
Figures

Figure 1. Original summary recommendations of the ACR TIRADS 2017
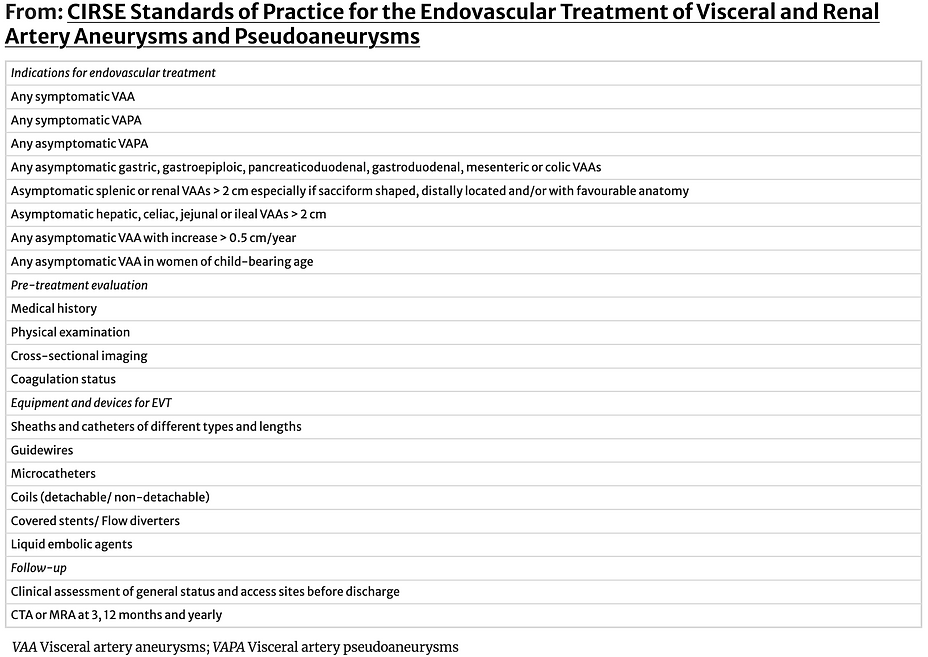
Figure 1. Original summary recommendations of the ACR TIRADS 2017
References
Risk of neoplasia
TI-RADS 1: < 2%
TI-RADS 2: < 2%
TI-RADS 3: 5%
TI-RADS 4: 5 to 20%
4 points: 6%
5 points: 10%
6 points: 13%
TI-RADS 5: ≥ 20%
Report 3 dimensions of the nodule
Include nodule halo if present
Recommendation according to longest diameter
No ultrasound follow-up for <1 year
Except for proven cancer requiring monitoring
If nodule already biopsied, classify TIRADS on ultrasound as usual
No specific recommendations in the report
Mention that management should be at least partly guided by biopsy results
If the nodule has already been biopsied with benign pathology and continues to increase on ultrasound,
According to ATA 2015, highly suspicious nodule should be followed up by ultrasound and cytology if necessary
Follow-up may be >5 years if remains below cytology threshold
References
Tessler FN, Middleton WD, Grant EG. Thyroid Imaging Reporting and Data System (TI-RADS): A User's Guide. Radiology [Internet]. 2018;287(1):29–36. doi:org/10.1148/radiol.2017171240
American College of Radiology. ACR Thyroid Imaging Reporting & Data System (TI-RADS) [Internet]. Acr.org. 2024. [ Link ]
WEBINARS
On Medusa : TIRADS and cervical mapping (SRQ 2020)